
Atrial Fibrillation (AFib) Diagnosis And Treatments Need a New Holistic Approach

Atrial Fibrillation (AF), is the most common heart disease nowadays, affecting around 7.6 million people only in the EU, most of whom are over 65 years old. One would think that given the large amount of studies dedicated to AF, it would be easy to diagnose, and yet we still fall short when it comes to identifying this underlying illness in patients. Not only that, current therapies still have a long way to go, as approximately only 60% are found to be effective.
This pressing issue becomes more apparent as we witness the steady rise of AF cases in the population.
So what is it that we know about AF? Why is it an important global health issue? Why are diagnoses and treatments not as effective as they should be, and what can be done about it?
- There are 3 underlying causes of AF: ‘wear and tear’ AF, congenital AF, and genetic AF
- AF severely affects patients’ quality of life
- Diagnostics and treatments are far from optimal because they are not directed at root causes of AF
- Doctors and patients should co-create AF research directed at root causes
The 3 types of AF: Wear and Tear, Congenital AF, and Genetic AF
So far, we know that AF can be subdivided into 3 different types based on the underlying cause.
-
Wear and Tear AF
This refers to AF associated with the natural process of ageing, as well as Western diet and lifestyle-related risk factors. These being factors such as hypertension, diabetes, obesity, coronary artery diseases, and various non-cardiovascular diseases including chronic kidney and inflammatory diseases.
-
Congenital AF
This refers to AF resulting to a combination of flaws in: genetics and/or the earliest stage of pregnancy, and factors surrounding surgical procedures needed to repair the heart defect. This type of AF often shows up at a younger age and rapidly progress from paroxysmal to persistent, and finally permanent AF.
-
Genetic AF
This refers to the 15% of AF patients who develop the condition due to a genetic predisposition (gene mutation), meaning it runs in the family.
Currently, the symptoms caused by wear and tear, congenital, and genetic AF, have only been partly understood, interpreted, and clarified.
AF and its effects on quality of life
It is very important that the causes and symptoms of AF are better understood because it truly is a matter of global health. Approximately 7.6 million people are severely affected by this condition in the EU. AF is, after all, associated with serious complications such as stroke, heart failure, cognitive impairment, and sudden cardiac arrest. All of which results in increased morbidity and mortality and poor health-related quality of life (QOL) and high health-care costs. The goals of health-care providers are to alleviate AF symptoms, reduce the risk of long-term sequelae, reduce mortality and improve QOL of the patient. Interestingly, physicians rate patient QOL higher than patients with AF do. The discordance is mainly found in patients with depression, sleep disorders and physical inactivity. To overcome this discordance, recent global initiatives designed standardized approaches to report on outcomes of quality of care and QOL based on patient-reported outcome measures (PROMs). PROMs facilitate the assessment of QOL of patients with AF, which serves to inform their health-care providers on the quality of care. The outcomes that matter most to patients with AF include emotional, cognitive and physical functioning, exercise tolerance, symptom severity, and ability to work. By implementing PROMs in the quality of care and life of AF patients, a holistic standardized outcome set for integration into routine clinical practice is realized.
Shortcomings of diagnosis and treatments in AF
Right now, diagnosis and treatments are not directed at the root causes of AF, and as such, fail to be as effective as they need to be. Treatments often follow a ‘one size fits all approach’. While they may alleviate symptoms, most treatments don’t manage to prevent AF progression from recurrent intermittent episodes (paroxysmal) to (longstanding) persistent and finally permanent AF.
For example, 70% of the patients with persistent AF who go through the invasive isolation therapy of the pulmonary veins, saw their AF resurface within one year and required multiple procedures. Also, the medicine available originated from the 1960s, and isn’t directed at the root causes of AF. This results in a failure to prevent AF progression in 85% of patients.
The need for co-creation of research directed at root causes of AF
Although there are many studies that have identified new possible drugs that might attack the root causes of AF, a pipeline with said new drugs is not available. Instead, the lack of knowledge on how AF develops in individual patients and consequential unpredictability of said patient’s response to AF therapy, ends up with treatments based on ‘trial-and-error’.
On top of that, much of the current medication available has potentially severe and life-threatening side effects, which causes many patients to decide not to take it.
This goes to show the desperate need for an understanding of AF in individual patients, and subsequent personalised treatment modalities.
Importantly, researchers within AFIP recognised that AF patients have important insights in disease triggers and ways to stop this arrhythmia. Patient insight has so far not been implemented in AF research. Via the recently granted project CIRCULAR by the Dutch Research Council (NWO) experience of patients shared via AFIP are incorporated in citizen science, experimental and clinical drug studies directed at molecular root causes of AF.
AFIP advocates improved collaboration between doctors and patients, in order to co-create AF research directed at root causes. This can then be used to design patient-tailored diagnostic tools and innovative therapies based on holistic AF management.
In short…
What’s clear is that there needs to be a shift in the approach to diagnosis and treatments of Atrial Fibrillation towards more holistic and inclusive methods, because it affects a very large portion of the population and truly has a severe impact in people’s lives. Only then can we really find a way to tackle AF at its core as an illness, rather that attempt to make its symptoms milder.
Do you know someone who might be interested in this?



Related articles

Atrial Tissue Conductivity Estimation For Analysis of Atrial Fibrillation
The Electrical Circuit of The Heart Have you ever considered your heart as an electrical circuit? That is how we, electrical engineers at TU Delft, look at the heart. To

Complaints After Ablation? This is The Explanation!

In several patients with atrial fibrillation (AFib), complaints return after ablation. This can be very frustrating and for a long time, this could not be explained well. For this reason,
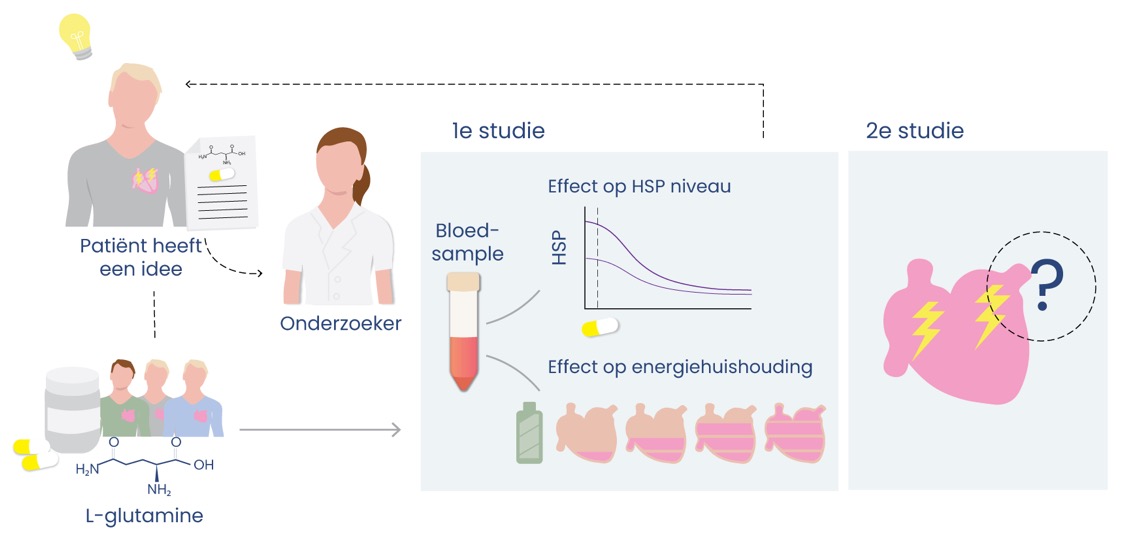
L-glutamine alters HSP levels and normalises energy status in patients with atrial fibrillation
Treatment strategies for atrial fibrillation (AF) are only moderately effective and do not prevent AF onset and progression. This difficulty of treatment predicts a great need to dissect root causes